
Useful Links and Numbers
During the last few months, I have been shared a lot of information that you may find useful. This ranges from being able to identify skin cancer early through to getting support, including financial assistance should this be needed. I have added some links and contact numbers below in case any of these are of use for you.
Skin Cancer Awareness:
Macmillan Cancer Support
Macmillan Cancer Support – Contact Us
0808 808 0000
NHS Test and Next Steps
Melanoma Focus
Melanoma Focus – Contact Us
0808 801 0777
Melanoma UK
Cancer Research UK
British Association of Dermatologists
Skin Cancer Support:
Macmillan Cancer Support
Macmillan Cancer Support – Contact Us
0808 808 0000
Melanoma UK
Maggies
Maggies – Find a centre
Shine Cancer Support
Shine Cancer Support – Contact Us
07804 479 413
Financial Assistance/advice:
Macmillan Cancer Support
Macmillan Cancer Support – Contact Us
0808 808 0000
Medical Exemption certificate
Employment and Support Allowance (ESA)
Personal Independence Payment (PIP)
Other:
Access Card
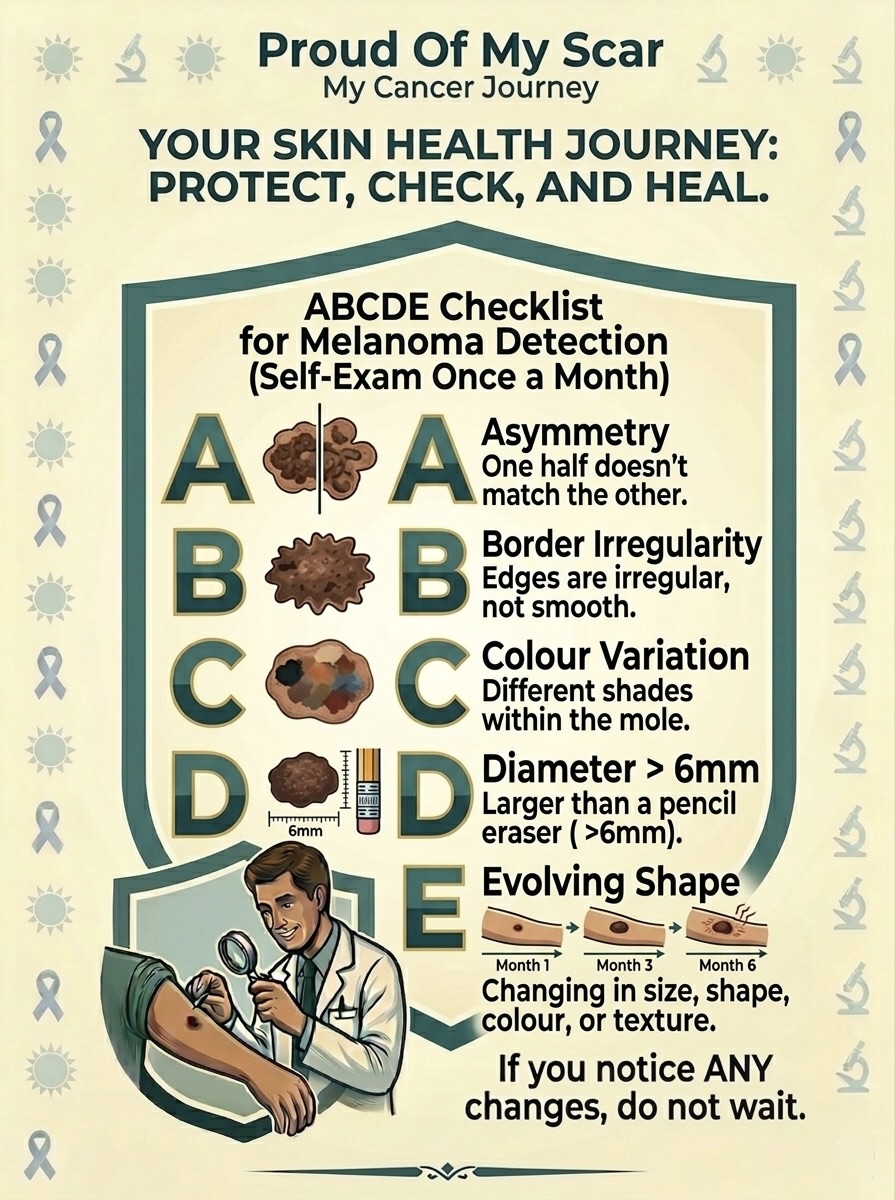
Protect and Check

ABCDE Checklist
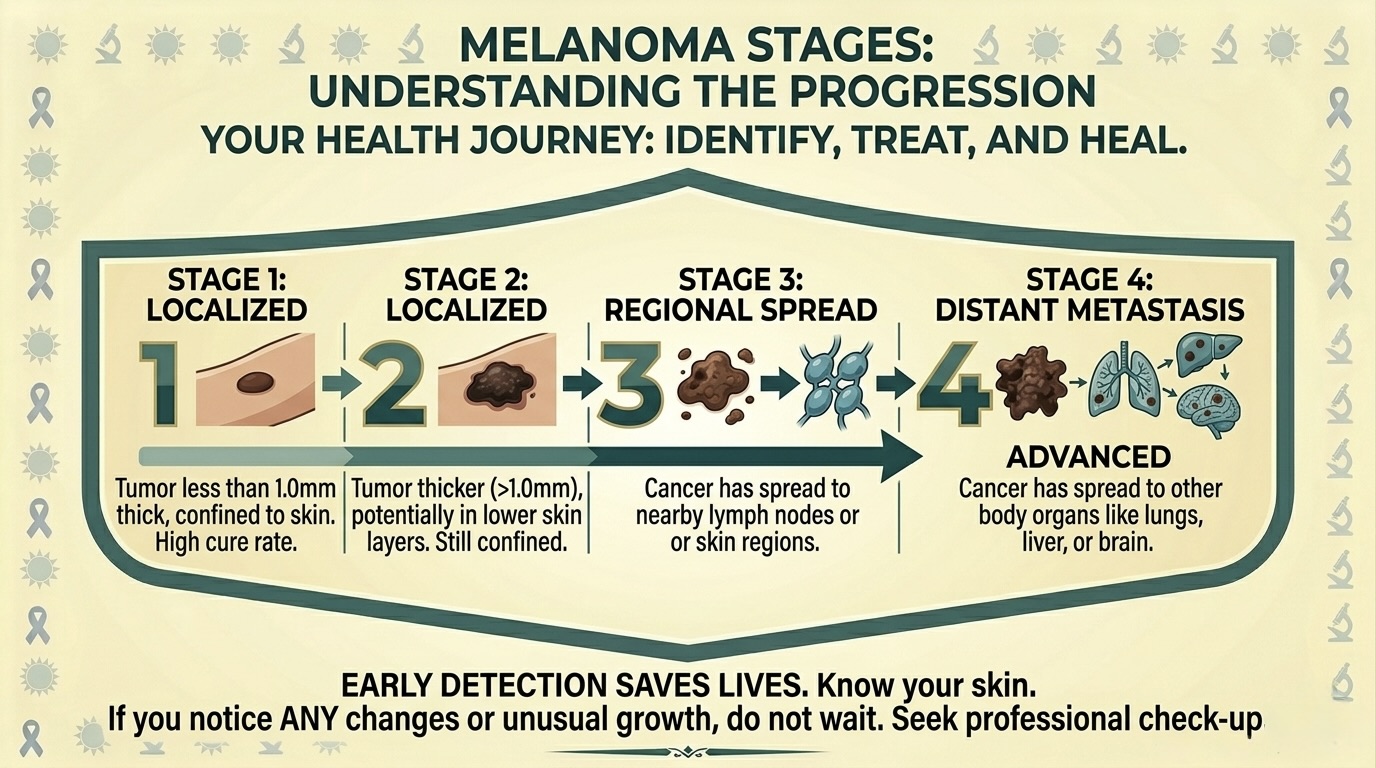
Melanoma Stages
If you have any concerns, always check with a medical professional as soon as possible.
Did you know
Melanoma causes:
• Almost 90% of all melanoma diagnosis is caused by exposure to Ultraviolet (UV) radiation
• Ultraviolet (UV) radiation can be caused by sunlight (e.g long exposure to the sun or bad sunburn), as well as artificial UV sources including tanning beds and sunlamps
• Other factors can influence the likelihood of developing melanoma including a history of sunburns, skin type, moles, genetics and age
• Some forms of melanoma can be caused by other factors beyond UV radiation, and can be common in people with darker skin tone, and are caused by genetic factors or internal cell mutations.
Melanoma Prevention
• Around 86% of melanoma cases are preventable. Although sunscreen is generally thought of as the best protection, this is not the only protection available.
• Clothing is your best defence. Sunscreen can easily rub off or not be applied correctly whereas clothing provides a consistent block to UV radiation. Look for clothing with an Ultraviolet Protection Factor (UPF) rating. Clothing with a UPF 50 rating ensures only 1/50th of the Sun’s UV radiation reaches your skin.
• If using sunscreen, ensure it protects against UVA (aging/Long-term damage) and UVB (burning). Look out for the star rating, 4 or 5 stars is recommended. Be mindful how long you spend in the sun, because wearing sunscreen can still result in melanomas.
• When applying sunscreen, be generous with the amount applied. Apply around 2 fingers worth for your face and neck, and apply enough sunscreen to fill a shot glass when applying to your body. As above, do be mindful that sunscreen can rub off, so ensure you are continually covered if you are not wearing clothing.
• Keep an eye out for your shadow. If your shadow appears shorter than you, this means that the sun’s UV rays are at their strongest, usually between 11am – 3om (UK). During this time, seek shade or stay indoors.
• Avoid artificial UV. The World Health Organisation has classed tanning beds as Group 1 Carcinogen, the same category as Tobacco. Likewise the UK government are introducing stricter regulations on commercial sunbeds due to melanoma risks.
Cancer Research stats:
• In the UK, approximately 18,300 people are diagnosed with melanoma every year. That’s about 48 cases every day
• 86% of melanoma cases are preventable
• Melanoma is the 5th most common cancer for females with around 9,000 new cases every year
• The most common location for melanoma in females is in the lower limb
• Melanoma is the 4th most common cancer for males with around 9,300 new cases every year
• The most common location for melanoma in males is in the trunk
• There could be around 26,500 new cases of melanoma skin cancers by 2040
• Around 25% of cases are people aged under 50 years old, whilst people aged 85-89 have the highest rate of diagnosis
• 92% of people diagnosed with melanoma survive melanoma for 10 years or more
• Over the last decade, melanoma incidence rates have increased by 25%. Females rates have risen by 22% and males by more than 29%.
Statistics source: Cancer Research UK, Melanoma skin cancer statistics Accessed April 2026
Survival rates:
| Stage | 5 Year | 10 Year |
| Stage 1A | 99% | 98% |
| Stage 1B | 97% | 94% |
| Stage 2A (w/surgery) | 94% | 88% |
| Stage 2B (w/surgery) | 87% | 82% |
| Stage 2C (w/surgery) | 82% | 75% |
| Stage 3A (w/surgery) | 93% | 88% |
| Stage 3B (w/surgery) | 83% | 77% |
| Stage 3C (w/surgery) | 69% | 60% |
| Stage 3D (w/surgery) | 32% | 24% |
Non-recurrence stats:
| Stage | Free after 5 Years |
| Stage 2B (w/adjuvant treatment) | 92% |
| Stage 2C (w/adjuvant treatment) | 89% |
| Stage 3A (w/adjuvant treatment) | 96.5% |
| Stage 3B (w/adjuvant treatment) | 91.5% |
| Stage 3C (w/adjuvant treatment) | 84.5% |
| Stage 3D (w/adjuvant treatment) | 66% |
Statistics source: Melanoma Focus, Survival rates by melanoma stage & Adjuvant treatment guide by melanoma stage Accessed April 2026
Terminology
You may hear a lot of unfamiliar terms if you are suspected of having/confirmed to have Skin Cancer. So I thought it may be useful to summarise some of these below for you. (click to open)
Melanoma Skin Cancer:
Melanoma, also called malignant melanoma, is a cancer that usually starts in the skin. It can start in a mole or in normal-looking skin.
The first symptom of melanoma skin cancer is usually a change in the shape, colour or size of a mole.
A superficial spreading melanoma is the most common type of melanoma. It is most often found on the arms, legs, chest and back. The melanoma cells usually grow slowly at first and spread out across the surface of the skin.
A nodular melanoma is the second most common type of melanoma. It can grow more quickly than other melanomas. It is also more likely to lose its colour when growing – becoming red rather than black. It is more commonly found on the chest, back, head or neck.
A Lentigo maligna melanoma is less common. It is usually found in older people, in areas of skin that have had a lot of sun exposure, such as the face and neck. It develops from a slow-growing, pre-cancerous condition called a lentigo maligna. Lentigo maligna is only in the upper layer of skin called the epidermis. It is sometimes called an insitu melanoma.
A acral lentinginous melanoma is rare. It is usually found on the palms of the hands, soles of the feet, or under fingernails or toenails. It is more common in people with black or brown skin. It is not thought to be caused by sun exposure.
Other rare types of melanoma include:
Malignant blue naevus
Desmoplastic melanoma
Amelanotic melanoma
Spitzoid melanoma
Treatment for Melanoma Skin Cancer:
Biopsy: Your doctor might remove the abnormal area to find out if it’s a melanoma skin cancer.
Common Biopsy Types
Shave/Saucerization Biopsy: A razor-type tool is used to remove a superficial area or “scoop” out the lesion, though it must be deep enough to avoid cutting through the tumour.
Excisional Biopsy (Preferred): The entire suspicious mole is removed with a scalpel, allowing the pathologist to examine the whole sample and determine the tumour’s depth (Breslow thickness).
Incisional Biopsy: Only a part of the lesion is removed. This is generally reserved for large, irregular lesions where removing the whole area immediately is not feasible.
Punch Biopsy: A circular tool removes a core sample of skin. Usually used if the lesion is small (3-5 mm) or for deeper, smaller samples.
Wide local excision: After the biopsy, you normally have a second operation to remove more tissue if you’re diagnosed with melanoma. Your doctor removes a larger area of healthy skin and tissue around where the melanoma was. This helps to reduce the risk of the melanoma coming back.
Sentinel lymph node biopsy (SLNB): Performed during the Wide local excision, as a way of checking the lymph nodes closest to the melanoma. You may have this test even if your lymph nodes do not look or feel swollen. It can help to find very small amounts of melanoma that have spread to the lymph nodes.
Adjuvant therapy: An additional treatment given after the primary treatment (usually surgery) to lower the risk of the cancer returning. Adjuvant therapy is offered either via targeted therapy or immunotherapy.
Targeted therapy: Is offered if the melanoma contains a BRAF mutation. It targets the abnormal or faulty BRAF protein. It is taken as capsules and tablets daily for a year
Immunotherapy: The immune system protects the body against illness and infection. Immunotherapies are treatments that use the immune system to recognise and kill cancer cells. It is administered via drip every 3, 4 or 6 weeks for a year.
Scans – Pre/Post surgery:
Sentinel lymph node scan: A harmless amount of radioactive liquid is injected into the area where the melanoma started. The radioactive liquid travels through the skin’s lymphatic vessels. It drains into the lymph nodes closest to the melanoma. These are the sentinel lymph nodes.
You usually then have a scan using a special camera. It finds the nodes that picked up the radioactivity and shows them on a screen. The skin is marked over the sentinel node or nodes to help the surgeon find them easily and remove them. The scan finds the sentinel nodes but cannot show whether melanoma cells are in the lymph nodes.
CT scan: Should any cancer cells be found, you may be asked to attend a CT scan. A CT scan uses x-rays to build a detailed picture of the inside of the body.
MRI scan: Should any cancer cells be found, you may be asked to attend an MRI scan. A MRI scan uses magnetism to build up a detailed picture of areas of the body.
Doctors may use an MRI scan to find out:
-The size of a cancer and whether it has spread.
-Whether a lump or abnormal area is cancer
